
Prevalence and Incidence Research

Granting wishes globally, informed by trusted health data
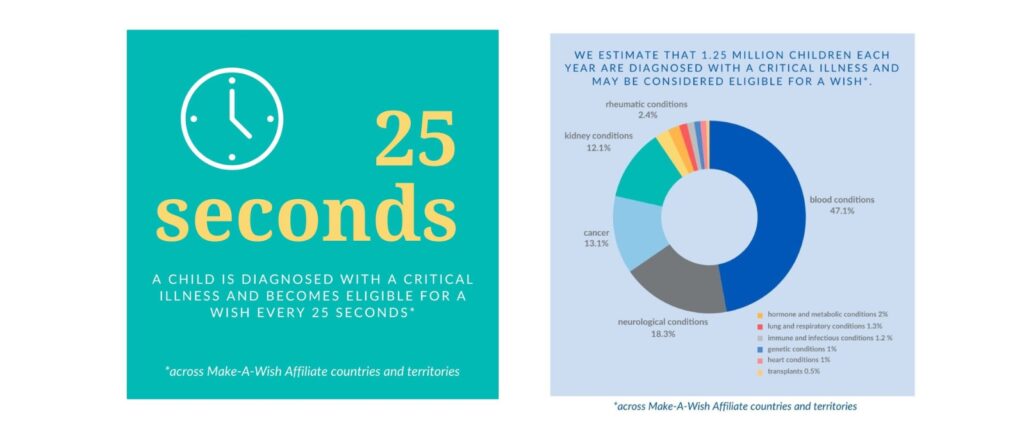
For the first time, Make-A-Wish International can present country-specific data on children who are eligible to have their wishes granted. This locally relevant, globally consistent data serves as the backbone for the definition and deployment of Make-A-Wish International’s strategic plan and will also support the strategies of its Affiliates.
This landmark research may be used to: Inform growth plans and strategies, Identify potentially underserved populations, Guide medical outreach and relationship building, Anticipate wish demand, Build credibility and trust and Support fundraising efforts.
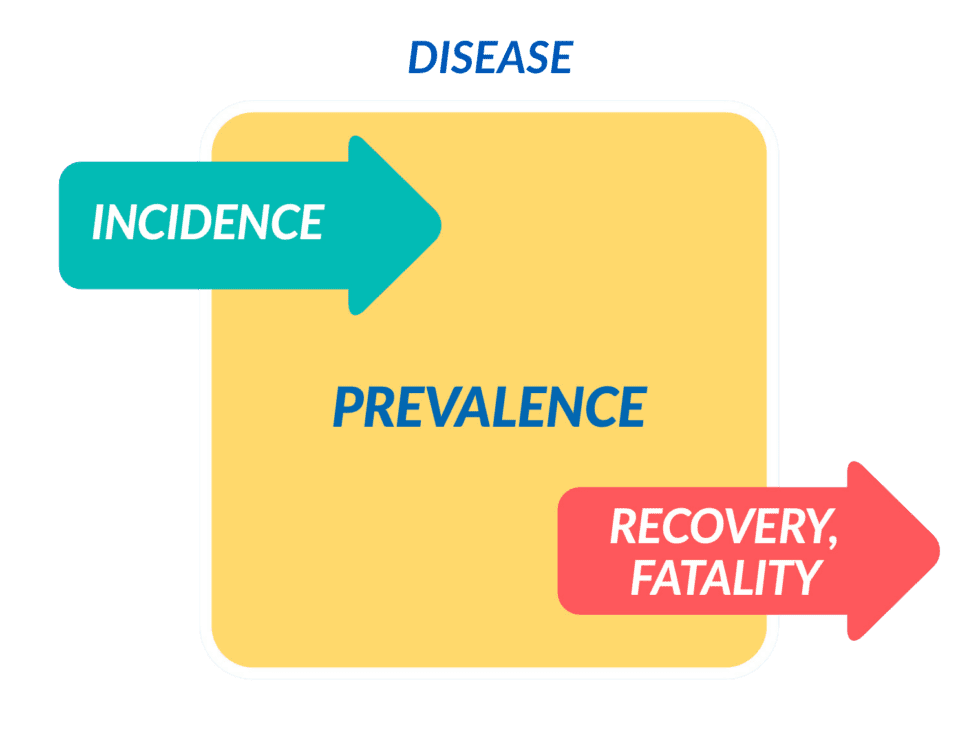
Prevalence vs. Incidence
- Prevalence is the number of individuals in a population who have a specific disease at a specified period of time, regardless
of when they first developed or were diagnosed with it. - Incidence is the number of individuals in a population who develop a disease (i.e. new cases) in a specified time period.
- Recovery and fatality reflects the number of individuals that exit the disease pool over a specified time period.
Source: Harvard School of Public Health
About the Research
Research For Impact (RFI), a Singapore-based think tank, was awarded the project. In the project, we collaborated with the Institute for Health Metrics and Evaluation (IHME), a research institute working in global health statistics and impact evaluation located at the University of Washington. The Global Burden of Disease database (GBD) was utilized to create country-specific paediatric disease profiles for qualifying conditions. We would like to thank RFI for their commitment to excellence in the delivery of this research project. Thank you, Disney, for supporting this project.
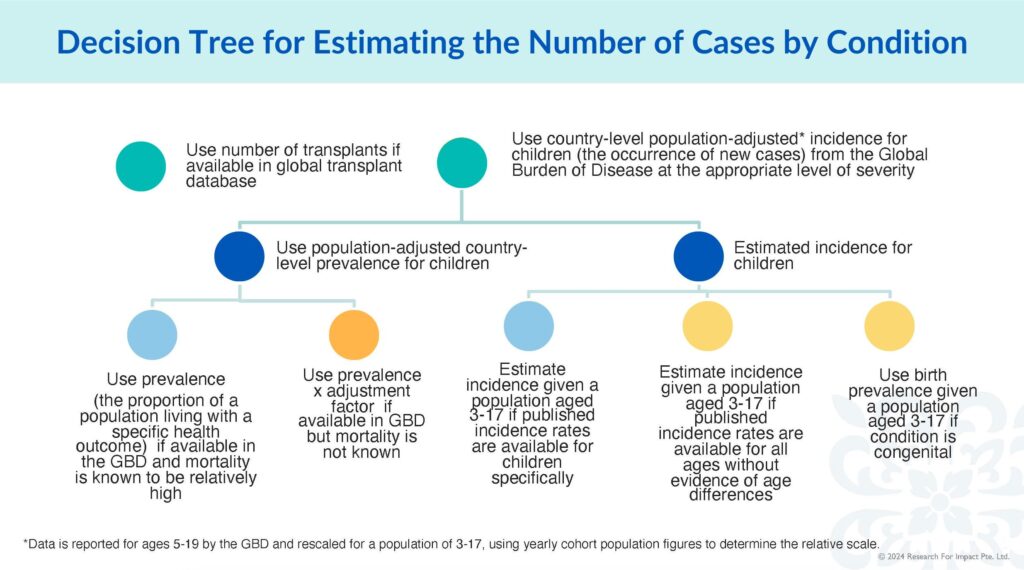
Summary of methodology
- The 2019 GBD data (the most recent available data) and the 2023 data on total wishes granted by Affiliates were used for this research.
- RFI conducted a comprehensive sift through the Global Burden of Disease Database for the conditions listed per our medical eligibility criteria.
- The International Medical Advisory Committee was also consulted to review and provide feedback on disease category/ condition inclusion and severity.
- To fill the data gaps, RFI looked through other global health data sources, including the World Health Organization, World Bank, OECD, and UNICEF.
- RFI also looked at the available disease registries and/or other relevant health databases of each country to gain a more comprehensive overview of the data.
- A scan of academic peer-reviewed literature was conducted to ensure coverage of rare diseases.
Download Overview of Research Results with Data per Affiliate (pdf)
Considerations and Assumptions
- In this project, while we work to match our data with our medical eligibility criteria as closely as possible, we are also conscious that data are collected differently across countries.
- Our primary data source, the GBD, collects information from various sources, including vital registration systems, health surveys, and disease registries. As data collection methods differ between countries, the GBD team standardises the data to ensure meaningful comparability. Once the data is standardised, complex statistical models are used to fill in data gaps, estimate health outcomes for various regions, ages, and sexes, and account for influencing factors, like population growth and ageing.
- The eligibility of individual children is determined with context specificity and case centricity in mind, taking into account the advice of the primary treating physician and the local medical advisory committee, as well as the condition of the individual child, within a set of common clinical areas that include, but are not limited to:
- Children whose current medical condition requires high-risk therapy to survive.
- Children who are dependent on technology to survive.
- Children with chronic conditions who demonstrate extreme long-term complications.
- Children at otherwise high risk of death.
- The eligible conditions are not clearly and consistently mapped to the International Classification of Diseases (ICD) or other codes and some of the information is scarce:
- A large number of rare / orphan diseases with very little information.
- Procedures (e.g. transplant) vs diseases.
- Missing data for some countries.